
A 59-year-old male without any medical history was brought to the emergency room with typical angina symptoms and the ECG of an inferior STEMI. Upon arrival, he had persistent symptoms and ST segment elevation in the inferior leads, but was respiratory and hemodynamically stable. He was directly transferred to the catheterization lab, where the team was expecting him.
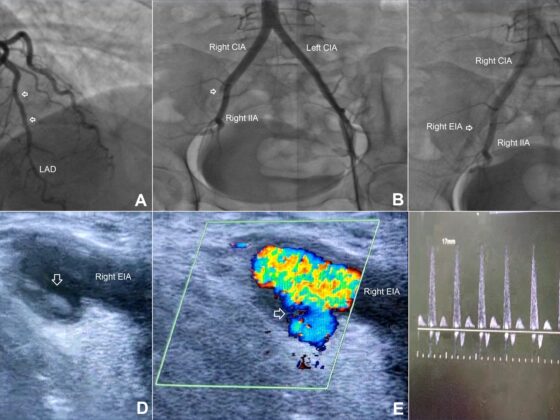
A right femoral approach was chosen (due to the pathological Allen test of the right radial artery). Surprisingly, the investigator was not able to pass the iliac artery with the J wire because of an extreme kinking of the arteries with several loops to be surpassed. He immediately changed the access to the left femoral artery hoping for better conditions. Unfortunately the left side offered similar challenges due to extreme kinking. Choosing a Terumo wire and carefully working his way up the descending aorta with the help of a diagnostic JR4 catheter, the investigator was then able to place a 45 cm kinking introducer sheath beyond the segment with extreme angulation. The angiography identified a thrombotic occlusion of the right coronary artery. All coronaries and especially the right one showed extreme tortuosity.
Performing the PCI of the right coronary artery proved to be similar challenging. The AL1 guiding catheter could not be manipulated to intubate the RCA. The JR4 catheter could only be brought to the vicinity of the ostium. Wiring the right coronary was therefore difficult. Luckily we were able to place the wire in the proximal RCA from “far away” after several attempts. The complete vessel wiring was also challenging due to the tortuosity and the constant displacement of the guiding catheter. A Guideliner catheter was used to stabilize the catheter position and also a balloon to facilitate wiring of the coronary. The PTCA and stenting were then successfully carried out. A DES (4,0x22mm) was implanted in the mid RCA. The final result was excellent with TIMI III flow. The door-to-balloon time was 35 minutes.
Difficult vascular access can complicate the course of emergency interventions. Keeping a bail out strategy and rescue measures in mind can save the day and also the patient.

Coronary
Victor Stefan
GERMANY
Double trouble STEMI
[kkstarratings]
You must belogged in to post a comment.